PERT
AI detection & classification of high-risk PE.
Modality:
CT Pulmonary Angiogram (CTPA)
Pathology:
Pulmonary Embolism
Status:
On hold

CSC Lead: Anil
This project is currently on hold due to resource and capacity issues and prioritisation of a different AI product. It will be picked up again soon.
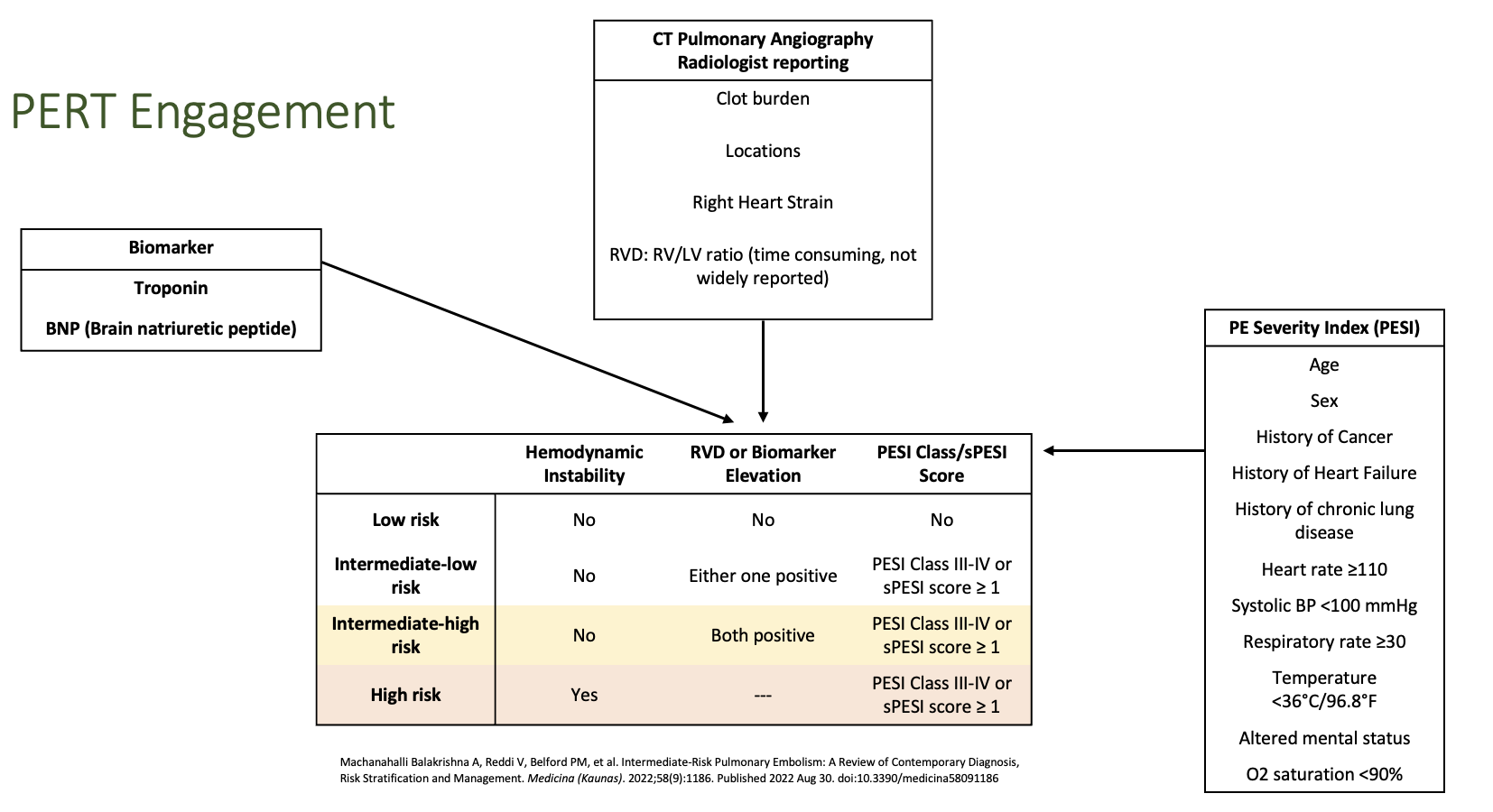
The Pulmonary Embolism Response Team (PERT) comprises Interventional Radiologists, Haematology consultants, Cardiothoracic surgeons, and Respiratory consultants,
Both patients arriving at GSTT, and in patients, with suspected High risk or intermediate-high risk PE will alert the PERT to allow multi-disciplinary decisions to be made for management, triage and treatment. Reduction in the time to alert PERT of high-risk PE can result in reduced length of stay, morbidity and improved patient outcomes from MDT decisions.
Clinical lead: Narayan Karunanithy, Karen Breen
Rationale
Triggering PERT, if the patient is not high risk, may benefit intermediate-high risk patients, however the speed of results to assign that risk category to a patient could cause delays in triggering that alert. An AI application is being evaluated to automatically pull CTPA images and calculate the right ventricular/left ventricular (RV/LV) ratio as a good indicator of right heart strain, to risk stratify patients above a certain threshold as appropriate to alert the PERT, therefore speeding up the CTPA reporting and subsequent PERT engagement towards better patient outcomes.
Patient pathway
Testing data
Approximately 4000 labelled CTs have been identified for retrospective testing of the commercial solution. Prospective trial will follow after if retrospective study demonstrates sufficient accuracy.
Goals
Automated classification of high and intermediate-high risk PE patients by accurately calculating Right Heart Strain (RV/LV ratios) from CTPAs.
Success criteria
Improvement in diagnostic accuracy and speed. Increased identification of intermediate risk patients alerting the PERT.